Valve Replacement
Valve replacement is a procedure to swap a damaged or diseased heart valve with a new mechanical or biological tissue valve. By 2026, technology has advanced…
- Success rate
- 93%-100%
- Avg cost (US)
- $80,000–$100,000 (range)
- Recovery
- 3–30 days (range)
- US volume / yr
- 150,000–300,000 (range)
Browse verified cardiology providers who offer this procedure.
This procedure is for individuals experiencing heart valve disease, such as aortic stenosis or mitral regurgitation. It helps those with symptoms like shortness of breath, chest pain, and fatigue, including high-risk patients and nonagenarians who previously might not have been candidates for surgery.
Depending on the approach, patients may undergo traditional surgery or a transcatheter procedure (like TAVR or TMVR). While traditional surgery involves a larger incision, minimally invasive options use smaller openings. Recent data shows high procedural success rates, particularly in transcatheter mitral repairs where device success can reach 100%. Patients will be monitored closely for heart rhythm and valve function immediately following the placement of the new device.
Recovery varies by procedure type. Minimally invasive methods typically offer shorter hospital stays and quicker returns to daily activities compared to open-heart surgery. For elderly patients, 30-day heart failure readmission rates are as low as 5%, though full recovery depends on the patient's age and overall health.
Estimated costs for specific transcatheter mitral procedures are approximately $87,724, though total expenses vary based on the type of valve and surgical approach used.
Questions to ask your doctor
- Am I a candidate for a minimally invasive or transcatheter valve replacement?
- Should I receive a mechanical valve or a biological tissue valve?
- What are my specific risks for heart failure readmission within the first year?
- How long do you expect my hospital stay to be based on the chosen surgical method?
- What is the expected lifespan of the replacement valve being used?
Frequently asked
Yes. Studies show that nonagenarians can benefit from transcatheter replacements with low 30-day heart failure readmission rates similar to younger patients.
Research indicates a high one-month survival probability, estimated at approximately 0.93 for these specific procedures.
Minimally invasive options generally involve less pain, shorter hospital stays, and a faster overall recovery compared to traditional open-heart surgery.
Recent outcomes show very high success, with up to 100% of patients achieving significant reduction in regurgitation at the one-year mark.
Deep dive: Heart Valve Replacement in 2026: Latest Recovery & TAVR Trends
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Please consult with a qualified healthcare professional regarding any medical conditions or treatments.
The heart is a masterpiece of engineering, but like any mechanical system, its components can wear down over time. At the center of this system are four valves that ensure blood flows in the right direction. When these valves become stiff (stenosis) or leaky (regurgitation), the heart has to work overtime, leading to fatigue, chest pain, and long-term damage. While 2026 brings us more non-surgical options than ever before, understanding the landscape of valve replacement is essential for anyone facing a diagnosis of valvular heart disease.
Who it's for
Valve replacement is typically recommended for patients whose heart valves are no longer functioning well enough to support healthy blood circulation. In the past, this was often seen as a condition of the elderly, but modern cardiology recognizes several distinct groups who benefit from this procedure.
The most common candidates are those with aortic stenosis—a buildup of calcium that narrows the valve opening—often seen in patients over 65. However, younger patients born with congenital issues, such as a bicuspid aortic valve (where the valve has two leaflets instead of three), frequently require replacement in their 40s or 50s.
You may be a candidate if you experience "heart failure" symptoms, such as shortness of breath during light activity, persistent swollen ankles, or dizzy spells. Doctors also use advanced imaging to identify "asymptomatic" patients whose valves are failing so severely that the heart is beginning to enlarge, even if the patient feels "fine." In 2026, the trend has shifted toward earlier intervention to prevent permanent heart muscle scarring.
How it works
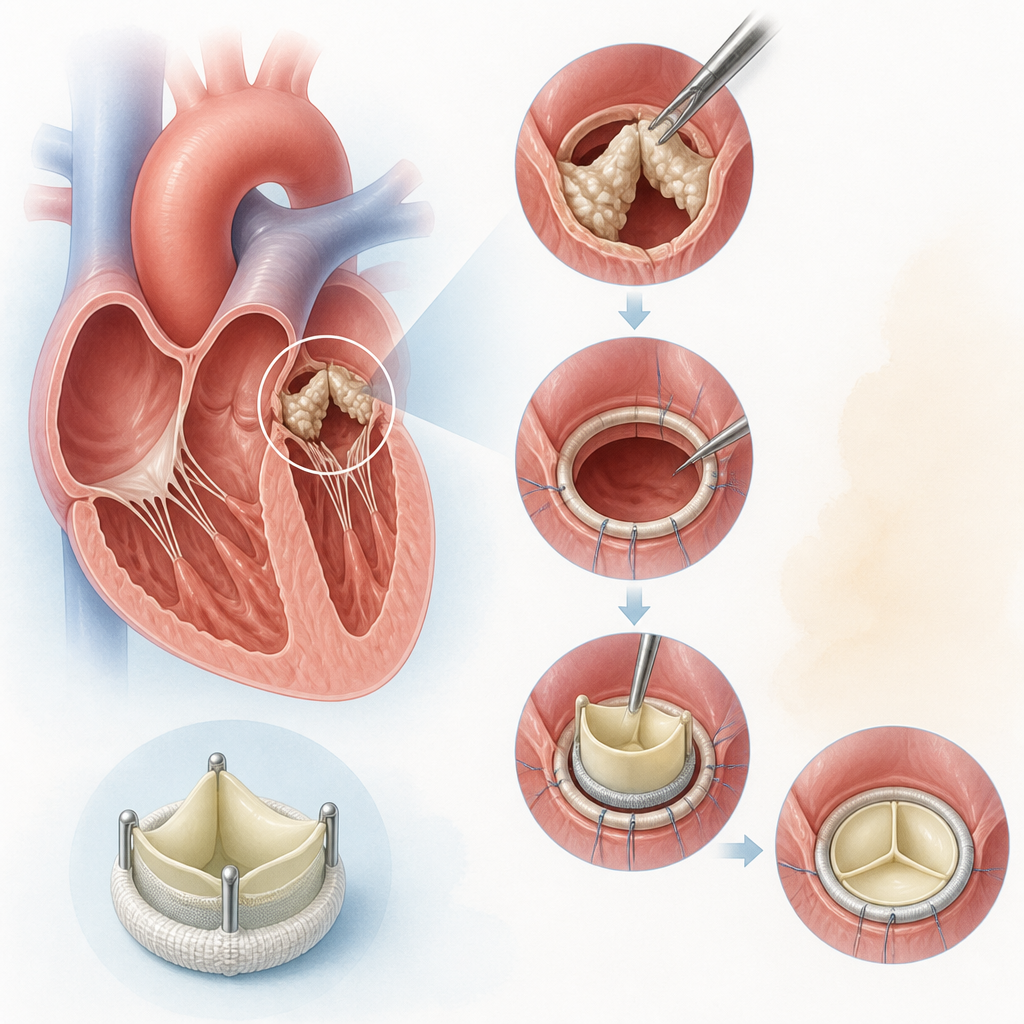
The way we replace valves has evolved dramatically. Today, there are two primary approaches: traditional surgical replacement and minimally invasive "transcatheter" replacement.
Traditional Surgical Valve Replacement involves a surgeon making an incision to access the heart directly. While it sounds daunting, it remains the "gold standard" for younger patients because it allows the surgeon to physically remove all calcium and ensure the most durable fit. During this procedure, the old valve is removed and replaced with either a mechanical valve (made of carbon and metal) or a biological tissue valve (made from porcine or bovine tissue).
Transcatheter Aortic Valve Replacement (TAVR) or Mitral Valve Replacement (TMVR) has become the preferred choice for many in 2026. This is a "keyhole" procedure where a new, collapsible valve is guided through a small tube (catheter), usually starting in the groin, up to the heart. Once inside the old valve, the new one is expanded, pushing the old leaflets aside and taking over the job immediately. These procedures often take less than an hour and require no large incisions.
The choice of valve material is also crucial. Mechanical valves can last a lifetime but require you to take blood-thinning medication forever. Biological valves don’t require long-term blood thinners but may need to be replaced again in 12 to 15 years.
Recovery & timeline
Recovery varies significantly based on the technique used.
For TAVR/TMVR (Minimally Invasive): Most patients are up and walking within six hours of the procedure. You will likely spend one night in the hospital for observation. By day three, most people can manage light household tasks. By week two, many are cleared to drive and return to sedentary work. Full internal healing usually takes about 30 days.
For Surgical Replacement: The hospital stay is typically four to seven days. Because the chest bone (sternum) needs time to knit back together, you will have "sternal precautions" for about six weeks—this means no lifting anything heavier than a gallon of milk. Full recovery, where you feel "back to yourself" or even better, usually occurs around the three-month mark.
Regardless of the method, in 2026, Cardiac Rehabilitation is a mandatory part of recovery. This is a structured exercise and education program that helps your heart adjust to its new, efficient valve.
Cost & insurance
In 2026, valve replacement is considered a standard of care and is covered by Medicare, Medicaid, and almost all private insurance plans, provided the medical necessity is documented through an echocardiogram or CT scan.
However, the "out-of-pocket" costs can vary. TAVR procedures often have a higher "sticker price" for the device itself, but because the hospital stay is shorter, the total bill may be lower than a week-long surgical stay. Most patients should expect to meet their annual deductible and out-of-pocket maximum.
It is important to check if your specific "Valve Clinic" is in-network. Many modern cardiology centers use a "Global Billing" model for 2026, which bundles the surgeon’s fee, the hospital stay, and the follow-up imaging into one estimate, making it easier for patients to plan financially.
Risks & alternatives
No procedure is without risk. For valve replacements, the primary concerns include bleeding, infection, and irregular heart rhythms (arrhythmias). A small percentage of patients (around 2-5%) may require a permanent pacemaker after the procedure if the new valve interferes with the heart's natural electrical pathways. Stroke risk, while significantly reduced by new "embolic protection" filters used during the procedure, remains a factor that your team will monitor closely.
Alternatives to replacement are becoming more common. If a valve is simply leaky (regurgitation) rather than narrowed, your doctor might suggest a "Valve Repair." This preserves your natural tissue using clips or rings. In 2026, medication therapy has also advanced; while medicine cannot "fix" a mechanical narrowing, new drugs can help manage the pressure on the heart to delay the need for surgery by months or years.
How to choose a provider
Choosing where to have your valve replaced is the most important decision in your journey. You should look for a "Heart Valve Center of Excellence." In 2026, the best centers utilize a "Heart Team" approach. This means your case isn't just seen by one surgeon; it is reviewed by an interventional cardiologist, a cardiac surgeon, and an imaging specialist who together decide the safest path for you.
Ask potential providers about their "volume"—research consistently shows that hospitals performing more than 100 valve replacements a year have significantly better outcomes and lower complication rates. Furthermore, ensure the facility uses the latest 3D-mapping technology, which allows them to "test fit" your valve digitally before the procedure even begins.
Finally, choose a provider who listens. A good cardiology team doesn't just look at your heart; they look at your lifestyle, your goals, and your long-term health to choose the valve that will give you the best quality of life for the next twenty years.
If you or a loved one are experiencing symptoms of heart valve disease, schedule a comprehensive cardiovascular evaluation with our specialist team today to discuss your replacement options.
Related patient questions
Sources
- Transcatheter aortic valve replacement over age 90: Risks vs benefits
- Aortic valve repair and aortic valve replacement - Mayo Clinic
- Cost-Effectiveness of Valve-in-Valve Transcatheter Mitral ... - PMC
- Outcomes of minimally invasive double valve surgery - PMC
- 1-Year Outcomes of Transfemoral Transcatheter Mitral Valve ...
Find a board-certified cardiology provider in your area.
General information only — not medical advice. Always consult a qualified clinician for your specific situation.